|
Overview
Differences between the lengths of the upper and/or lower legs are called leg length discrepancies (LLD). A leg length difference may simply be a mild variation between the two sides of the body. This is not unusual in the general population. For example, one study reported that 32 percent of 600 military recruits had a 1/5 inch to a 3/5 inch difference between the lengths of their legs. This is a normal variation. Greater differences may need treatment because a significant difference can affect a patient's well-being and quality of life.  Causes A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences. Symptoms As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies. Diagnosis Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all. Non Surgical Treatment Treatment depends on what limb has the deformity and the amount of deformity present. For example, there may be loss of function of the leg or arm. Cosmetic issues may also be a concern for the patient and their family. If there are problems with the arms, the goal is to improve the appearance and function of the arm. Treatment of leg problems try to correct the deformity that may cause arthritis as the child gets older. If the problem is leg length, where the legs are not "equal," the goal is equalization (making the legs the same length). Treatment may include the use of adaptive devices, prosthesis, orthotics or shoe lifts. If the problem is more severe and not treatable with these methods, then surgery may be necessary.  leg length discrepancy measurement Surgical Treatment Surgeries to lengthen a leg are generally only performed when there is a difference in leg length of greater than four centimeters. These types of surgeries can be more difficult and have more complications, such as infections, delayed healing, dislocations, and high blood pressure. In a several step process, bone lengthening surgeries involve cutting a bone in two in order to allow new bone growth to occur. After the bone is cut, a special apparatus is worn with pins that will pull the bone apart at approximately one millimeter per day. This causes osteogenesis, or new bone growth, in between the cut bone segments. A cast or brace may be required for several months after surgery to allow the new bone growth to harden and provide extra support. Overview
 Heel pain is a problem for many people. It makes standing and even walking around for long periods of time very uncomfortable. Several different conditions can lead to uncomfortable heels, but the most common culprit is plantar fasciitis. This is the inflammation and swelling of the plantar fascia, a tendon that runs along the sole of your foot and attaches to the bottom of the calcaneus, or heel bone. Repeated hard impacts or strain from overuse causes micro-tears to develop in the tendon, irritating it. The minor damage compounds over time and causes the tissue to swell and tighten, painfully pulling on the heel bone. Causes Heel pain is not usually caused by a single injury, such as a twist or fall, but rather the result of repetitive stress and pounding of the heel. The most common causes of heel pain are Plantar fasciitis (plantar fasciosis) - inflammation of the plantar fascia. The plantar fascia is a strong bowstring-like ligament that runs from the calcaneum (heel bone) to the tip of the foot. When the plantar fasciitis is stretched too far its soft tissue fibers become inflamed, usually where it attaches to the heel bone. Sometimes the problem may occur in the middle of the foot. The patient experiences pain under the foot, especially after long periods of rest. Some patients have calf-muscle cramps if the Achilles tendon tightens too. Heel bursitis, inflammation of the back of the heel, the bursa (a fibrous sac full of fluid). Can be caused by landing awkwardly or hard on the heels. Can also be caused by pressure from footwear. Pain is typically felt either deep inside the heel or at the back of the heel. Sometimes the Achilles tendon may swell. As the day progresses the pain usually gets worse. Heel bumps (pump bumps) common in teenagers. The heel bone is not yet fully mature and rubs excessively, resulting in the formation of too much bone. Often caused by having a flat foot. Among females can be caused by starting to wear high heels before the bone is fully mature Tarsal tunnel syndrome, a large nerve in the back of the foot becomes pinched, or entrapped (compressed). This is a type of compression neuropathy that can occur either in the ankle or foot. Chronic inflammation of the heel pad, caused either by the heel pad becoming too thin, or heavy footsteps. Stress fracture, this is a fracture caused by repetitive stress, commonly caused by strenuous exercise, sports or heavy manual work. Runners are particularly prone to stress fracture in the metatarsal bones of the foot. Can also be caused by osteoporosis. Severs disease (calcaneal apophysitis) the most common cause of heel pain in child/teenage athletes, caused by overuse and repetitive microtrauma of the growth plates of the calcaneus (heel bone). Children aged from 7-15 are most commonly affected. Achilles tendonosis (degenerative tendinopathy) also referred to as tendonitis, tendinosis and tendinopathy. A chronic (long-term) condition associated with the progressive degeneration of the Achilles tendon. Sometimes the Achilles tendon does not function properly because of multiple, minor microscopic tears of the tendon, which cannot heal and repair itself correctly, the Achilles tendon receives more tension than it can cope with and microscopic tears develop. Eventually, the tendon thickens, weakens and becomes painful. Symptoms The symptoms of plantar fasciitis are pain on the bottom of the heel, pain in the arch of the foot, pain that is usually worse upon arising, pain that increases over a period of months. People with plantar fasciitis often describe the pain as worse when they get up in the morning or after they?ve been sitting for long periods of time. After a few minutes of walking the pain decreases, because walking stretches the fascia. For some people the pain subsides but returns after spending long periods of time on their feet. Diagnosis After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests. Non Surgical Treatment The following steps may help relieve your heel pain. Use crutches to take weight off your feet. Rest as much as possible for at least a week. Apply ice to the painful area. Do this at least twice a day for 10 to 15 minutes, more often in the first couple of days. Take acetaminophen or ibuprofen for pain. Wear proper-fitting shoes. Use a heel cup, felt pads in the heel area, or shoe insert. Wear night splints. Your doctor may recommend other treatments, depending on the cause of your heel pain. Call your doctor if your heel pain does not get better after 2 - 3 weeks of home treatment. Also call if your pain is getting worse despite home treatment. Your pain is sudden and severe. You have redness or swelling of your heel. You cannot put weight on your foot. Surgical Treatment Only a relatively few cases of heel pain require surgery. If required, surgery is usually for the removal of a spur, but also may involve release of the plantar fascia, removal of a bursa, or a removal of a neuroma or other soft-tissue growth. heel pads shoes too big Prevention  Wearing real good, supportive shoes are a great way to avoid heel pain. Usually, New Balance is a good shoe to wear, just for everyday shoe gear. By wearing proper footwear and performing thorough stretches, athletes can help prevent frequent heel pain. If you are starting to get a little discomfort or pain in the feet or heel, know that pain is not normal. So if you are having pain, you should be proactive and visit our office. If you let heel pain get out of control you could run into several other problems. It is always suggested to visit a podiatrist whenever you are experiencing pain. Overview
 Morton?s Neuroma is a pathological condition of the common digital nerve in the foot, most frequently between the third and fourth metatarsals (third inter-metatarsal space). The nerve sheath becomes abnormally thickened with fibrous (scar) tissue and the nerve fibres eventually deteriorate.This condition is named for the American surgeon, Thomas George Morton (1835-1903), who first recognised the condition in 1876. Incidentally his father was the dentist who discovered the anaesthetics; initially Nitrous oxide, the very gas used today in cryosurgery for the condition his son lent his name to? Morton?s neuroma. Morton?s Neuroma is a pathological condition of the common digital nerve in the foot, most frequently between the third and fourth metatarsals (third inter-metatarsal space). The nerve sheath becomes abnormally thickened with fibrous (scar) tissue and the nerve fibres eventually deteriorate.This condition is named for the American surgeon, Thomas George Morton (1835-1903), who first recognised the condition in 1876. Incidentally his father was the dentist who discovered the anaesthetics; initially Nitrous oxide, the very gas used today in cryosurgery for the condition his son lent his name to? Morton?s neuroma.Causes Wearing shoes that are too tight can make the pain of Morton's neuroma worse. This is because the toe bones are more likely to press on the affected nerve if your shoes are too tight. High-heeled shoes, particularly those over 5cm (2 inches), or shoes with a pointed or tight toe area, can also compress your toes and make the pain worse. This is why women tend to be affected by Morton's neuroma more than men. Foot conditions. Symptoms The symptoms of a Morton's neuroma are classic in nature. The patient complains of a burning , tingling, slightly numb feeling (dysesthesias) which radiates out to the toes on either side of the interspace that is involved. For instance, a Morton's neuroma of the third interspace will result in pain between the third and fourth toes, and a neuroma in the second interspace will cause pain between the second and third toes. The symptoms are usually aggravated by wearing shoes, particularly those with high heels. Symptoms are relieved by walking in flat, wide shoes or going barefoot. Rarely will the patient experience pain when sitting or laying down. Diagnosis The diagnosis of interdigital neuroma is usually made by physical examination and review of the patient's medical history.MRI ad High Definition Ultrasound examination may be useful to confirm the diagnoses however they may still not be 100% reliable. The commonest reason for this is de to natural substances present in between the metatarsal heads and between the fat pad and the intermetatarsal ligament. These natural substances i.e. bursa, fat, capsular thickening and even bony growths, can all be a factor in the impingement process and may need to be surgically cleared. Non Surgical Treatment Treatment depends on the severity of your symptoms. Your doctor will likely recommend trying conservative approaches first. Arch supports and foot pads fit inside your shoe and help reduce pressure on the nerve. These can be purchased over-the-counter, or your doctor may prescribe a custom-made, individually designed shoe insert, molded to fit the exact contours of your foot.  Surgical Treatment When early treatments fail and the neuroma progresses past the threshold for such options, podiatric surgery may become necessary. The procedure, which removes the inflamed and enlarged nerve, can usually be conducted on an outpatient basis, with a recovery time that is often just a few weeks. Your podiatric physician will thoroughly describe the surgical procedures to be used and the results you can expect. Any pain following surgery is easily managed with medications prescribed by your podiatrist. Prevention Ensuring that shoes are well fitted, low-heeled and with a wide toe area may help to prevent Morton's neuroma. There are two different kinds of leg length discrepancies, congenital and acquired. Congenital means that you are born with it. One leg is anatomically shorter in comparison to the other. As a result of developmental periods of aging, the brain senses the step pattern and identifies some variance. The body typically adapts by tilting one shoulder over to the "short" side. A difference of under a quarter inch is not really irregular, require Shoe Lifts to compensate and commonly does not have a serious effect over a lifetime.
 Leg length inequality goes typically undiscovered on a daily basis, yet this issue is very easily corrected, and can eliminate numerous cases of back ache. Treatment for leg length inequality typically involves Shoe Lifts. Most are very reasonably priced, frequently costing under twenty dollars, compared to a custom orthotic of $200 and up. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position. Lumbar pain is the most prevalent health problem afflicting men and women today. Over 80 million people experience back pain at some point in their life. It's a problem which costs businesses millions of dollars every year as a result of lost time and production. Fresh and better treatment solutions are continually sought after in the hope of lowering economic influence this issue causes.  People from all corners of the earth suffer from foot ache due to leg length discrepancy. In these cases Shoe Lifts might be of very helpful. The lifts are capable of eliminating any discomfort and pain in the feet. Shoe Lifts are recommended by many qualified orthopaedic practitioners". In order to support the body in a well-balanced fashion, your feet have got a vital job to play. Inspite of that, it's often the most neglected area in the body. Many people have flat-feet which means there is unequal force placed on the feet. This will cause other parts of the body like knees, ankles and backs to be impacted too. Shoe Lifts make sure that the right posture and balance are restored. There are not one but two different types of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is structurally shorter than the other. As a result of developmental stages of aging, the brain picks up on the stride pattern and recognizes some variation. Your body usually adapts by dipping one shoulder over to the "short" side. A difference of under a quarter inch is not blatantly excessive, demand Shoe Lifts to compensate and in most cases does not have a serious effect over a lifetime.
 Leg length inequality goes typically undiagnosed on a daily basis, yet this issue is easily corrected, and can reduce numerous instances of lumbar pain. Therapy for leg length inequality commonly consists of Shoe Lifts. These are typically very inexpensive, commonly priced at less than twenty dollars, compared to a custom orthotic of $200 if not more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Low back pain is the most widespread condition affecting people today. Around 80 million men and women have problems with back pain at some point in their life. It's a problem which costs employers millions of dollars year after year because of lost time and production. Innovative and superior treatment methods are constantly sought after in the hope of lowering economical influence this condition causes.  People from all corners of the world suffer from foot ache as a result of leg length discrepancy. In a lot of these cases Shoe Lifts are usually of very helpful. The lifts are capable of relieving any discomfort and pain in the feet. Shoe Lifts are recommended by numerous skilled orthopaedic physicians. So that they can support the body in a nicely balanced manner, the feet have got a crucial job to play. Despite that, it is often the most neglected area in the body. Some people have flat-feet meaning there may be unequal force exerted on the feet. This causes other areas of the body like knees, ankles and backs to be affected too. Shoe Lifts make sure that ideal posture and balance are restored. There are actually two unique variations of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is anatomically shorter compared to the other. As a result of developmental phases of aging, the brain senses the walking pattern and identifies some variation. The human body usually adapts by dipping one shoulder to the "short" side. A difference of under a quarter inch isn't blatantly irregular, require Shoe Lifts to compensate and commonly won't have a serious effect over a lifetime.
 Leg length inequality goes largely undiagnosed on a daily basis, yet this problem is simply solved, and can reduce quite a few instances of back discomfort. Treatment for leg length inequality usually involves Shoe Lifts. These are affordable, commonly priced at less than twenty dollars, in comparison to a custom orthotic of $200 or maybe more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Mid back pain is the most common condition affecting men and women today. Around 80 million men and women suffer from back pain at some point in their life. It is a problem that costs employers huge amounts of money year after year due to time lost and output. Fresh and superior treatment methods are continually sought after in the hope of minimizing the economic impact this issue causes. People from all corners of the world suffer from foot ache as a result of leg length discrepancy. In a lot of these situations Shoe Lifts can be of very beneficial. The lifts are capable of eliminating any discomfort and pain in the feet. Shoe Lifts are recommended by many specialist orthopaedic doctors. In order to support the human body in a balanced manner, feet have got a vital task to play. In spite of that, it can be the most neglected region of the body. Some people have flat-feet which means there is unequal force exerted on the feet. This will cause other body parts such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
Overview
 A bunion (hallux valgus) is an enlargement of the bone or tissue around a joint at the base of the big toe or at the base of the little toe (in which case it is called a "bunionette" or "tailor's bunion"). Bunions often occur when the joint is stressed over a prolonged period. Ninety percent of bunions occur in women, primarily because women may be more likely to wear tight, pointed, and confining shoes. Bunions may be inherited as a family trait. Bunions may also result from arthritis, which often affects the big toe joint. A bunion (hallux valgus) is an enlargement of the bone or tissue around a joint at the base of the big toe or at the base of the little toe (in which case it is called a "bunionette" or "tailor's bunion"). Bunions often occur when the joint is stressed over a prolonged period. Ninety percent of bunions occur in women, primarily because women may be more likely to wear tight, pointed, and confining shoes. Bunions may be inherited as a family trait. Bunions may also result from arthritis, which often affects the big toe joint.Causes There are many factors which can contribute to the development of a bunion. The common causes are genetic factors, poor foot mechanics, high-heeled or narrow footwear and trauma to the toe. It is believed that constant stress on the joint of the big toe causes mild displacement of the bones and the joint, along with thickening of the tissues and a change in the pull of the muscles. This can result in a degree of arthritis of the joint, and over time, further displacement of the toe. This may lead to pain, difficultly with fitting shoes and corns/calloused lesions due to excess pressure on the smaller digits. Symptoms Symptoms, which occur at the site of the bunion, may include pain or soreness, inflammation and redness, a burning sensation, possible numbness. Symptoms occur most often when wearing shoes that crowd the toes, such as shoes with a tight toe box or high heels. This may explain why women are more likely to have symptoms than men. In addition, spending long periods of time on your feet can aggravate the symptoms of bunions. Diagnosis Before examining your foot, the doctor will ask you about the types of shoes you wear and how often you wear them. He or she also will ask if anyone else in your family has had bunions or if you have had any previous injury to the foot. In most cases, your doctor can diagnose a bunion just by examining your foot. During this exam, you will be asked to move your big toe up and down to see if you can move it as much as you should be able to. The doctor also will look for signs of redness and swelling and ask if the area is painful. Your doctor may want to order X-rays of the foot to check for other causes of pain, to determine whether there is significant arthritis and to see if the bones are aligned properly. Non Surgical Treatment If abnormal pronation is identified and corrected early, the formation of a bunion can be prevented. However, if the bunion has already developed and cannot be tolerated by the patient, surgery is necessary. Amputation of the big toe ceased to be a treatment for bunions many generations ago, but only in the past few years have surgical procedures been developed to incorporate the realignment of the bone with the correction of the abnormal motion that led to deformity.  Surgical Treatment When the pain of a bunion interferes with daily activities, and conservative treatment has been completed it's time to discuss surgical options. Foot Mechanics has excellent relationships with many Orthopaedic Surgeons, who are the specialists who perform bunion surgery. Because bunions are caused by faulty foot mechanics surgery can improve the look of your feet by removing the ?bump? but if the underlying mechanics are not addressed then the bunion is likely to return. For this reason orthotics are used post-surgery to prevent the return of bunions. Prevention The best way to reduce your chances of developing a bunion is to wear shoes that fit properly. Any shoe that is too tight or too high will force your toes together and may cause the condition to develop. Shoes need to be wide enough, so they aren't rubbing against the joint, and preferably made of leather. Avoid shoes with a lot elaborate stitching at the front, as this can also cause irritation. Heels should be no more than three to four inches and you should only wear them occasionally. Court shoes should seldomly be worn, as they do not give the foot any support. Be honest with yourself, you know if your shoes aren't fitting you comfortably. Do something about it, or you will suffer for your vanity.
Overview
 When the Achilles tendon ruptures. it gets completely torn by a sudden movement of the ankle/leg. It usually occurs in a tendon that is worn out and has weakened over time and then suddenly tears when there is enough force. It typically occurs during recreational sports that involve running, jumping, and pivoting, such as basketball, soccer or racquet sports. It is most often seen in men in their 30s and 40s. Some medications and medical problems can predispose to having an Achilles rupture. When the Achilles tendon ruptures. it gets completely torn by a sudden movement of the ankle/leg. It usually occurs in a tendon that is worn out and has weakened over time and then suddenly tears when there is enough force. It typically occurs during recreational sports that involve running, jumping, and pivoting, such as basketball, soccer or racquet sports. It is most often seen in men in their 30s and 40s. Some medications and medical problems can predispose to having an Achilles rupture.Causes Ruptured Achilles tendons may result from falling from a height or down a hole. Increasing training intensity abruptly, boosting distance, frequency or duration by more than 10% a week. Failing to stretch before and after exercise. Repetitive training, especially uphill running. Deyhydration, which causes cramping and tightness in the calves. Taking antibiotics. Improper footwear. Explosive movements in competitive sports like basketball, soccer or track & field. Symptoms Many people say that a ruptured Achilles feels like ?being shot in the heel?, if you can imagine how enjoyable that feels. You may hear a snap sound or feel a sudden sharp pain when the tendon tears. After a few moments, the pain settles and the back of the lower leg aches. You can walk and bear weight, but you may find it difficult to point the foot downward or push off the ground on the affected side. You will be unable to stand on tiptoe. Bruising and swelling are likely, and persistent pain will be present. Similar symptoms may be caused by an inflamed Achilles tendon (Achilles tendonitis), a torn calf muscle, arthritis of the ankle, or deep vein thrombosis in the calf, so an MRI or ultrasound scan will likely be used to diagnose your condition. Diagnosis It is usually possible to detect a complete rupture of the Achilles tendon on the history and examination. A gap may be felt in the tendon, usually 4-5cm above the heel bone. This is the normal site of injury and is called an intra-substance tear. The tear can occur higher up about 10cm above the insertion into the heel at the site where the muscles join the tendon, this is known as a musculo-tendinous tear. A special test will be performed which involves squeezing the calf. Normally if the Achilles tendon is intact this causes the foot to point downwards but if it is ruptured it causes no movement. To confirm the diagnosis and the exact site of the rupture it may be necessary to perform an Ultra-sound or MRI scan. Non Surgical Treatment The most widely used method of non-surgical treatment involves the use of serial casting with gradual progression from plantar flexion to neutral or using a solid removable boot with heel inserts to bring the ends of the tendon closer together. The advantage of a solid removable boot is that it allows the patient to begin early motion and is removable. Wide variability exists among surgeons in regards to the period of absolute immobilization, initiating range of motion exercises, and progression of weight bearing status. 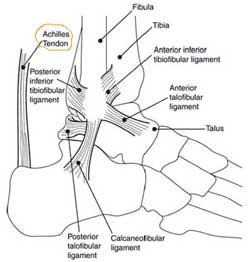 Surgical Treatment Surgery for Achilles tendon rupture requires an operation to open the skin and physically suture (sew) the ends of the tendon back together, has a lower incidence of re-rupture than nonsurgical treatment. Allows return to pre-injury activities sooner and at a higher level of functioning with less shrinkage of muscle. Risks are associated with surgery, anesthesia, infection, skin breakdown, scarring, bleeding, accidental nerve injury, higher cost, and blood clots in the leg are possible after surgery. Surgery has been the treatment of choice for the competitive athlete or those with a high level of physical activity, for those with a delay in treatment or diagnosis, and for those whose tendons have ruptured again. Prevention The following can significantly reduce the risk of Achilles tendon rupture. Adequate stretching and warming up prior to exercising. If playing a seasonal sport, undertake preparatory exercises to build strength and endurance before the sporting season commences. Maintain a healthy body weight. This will reduce the load on the tendon and muscles. Use footwear appropriate for the sport or exercise being undertaken. Exercise within fitness limits and follow a sensible exercise programme. Increase exercise gradually and avoid unfamiliar strenuous exercise. Gradual ?warm down? after exercising. Overview
Neuromuscular. Muscle imbalance causing different pull on pelvis (anterior superior Ilium or posterior inferior ilium). Muscle tightness/shortness especially piriformis (which lead to an external rotation of the femur thus shortening of the leg) and QL (raising ipsilateral iliac crest). Genu recurvatum, valgus, varus. Asymmetrical fallen arches or over pronation. Polio, Cerebral palsy. Trauma. Fracture. Injury epiphyseal plate. Iatrogenic (such as hip or knee surgery). Idiopathic. Hip disorder (such Legg-Perthes-Calve? or Slipped capital femoral epiphysis). Advanced degenerative changes. Causes Some limb-length differences are caused by actual anatomic differences from one side to the other (referred to as structural causes). The femur is longer (or shorter) or the cartilage between the femur and tibia is thicker (or thinner) on one side. There could be actual deformities in one femur or hip joint contributing to leg length differences from side to side. Even a small structural difference can amount to significant changes in the anatomy of the limb. A past history of leg fracture, developmental hip dysplasia, slipped capital femoral epiphysis (SCFE), short neck of the femur, or coxa vara can also lead to placement of the femoral head in the hip socket that is offset. The end-result can be a limb-length difference and early degenerative arthritis of the hip. Symptoms The most common symptom of all forms of LLD is chronic backache. In structural LLD the sufferer may also experience arthritis within the knee and hip are, flank pain, plantar fasciitis and metatarsalgia all on the side that is longer. Functional LLD sufferers will see similar conditions on the shorter side. Diagnosis Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis. Non Surgical Treatment Non-surgical treatment can be effective. A shoe lift may be recommended if the leg length difference is less than 1 inch. More significant leg length discrepancies may require a surgical procedure. In children, surgical procedures are available to help make leg lengths more equal.  Surgical Treatment Surgeries to lengthen a leg are generally only performed when there is a difference in leg length of greater than four centimeters. These types of surgeries can be more difficult and have more complications, such as infections, delayed healing, dislocations, and high blood pressure. In a several step process, bone lengthening surgeries involve cutting a bone in two in order to allow new bone growth to occur. After the bone is cut, a special apparatus is worn with pins that will pull the bone apart at approximately one millimeter per day. This causes osteogenesis, or new bone growth, in between the cut bone segments. A cast or brace may be required for several months after surgery to allow the new bone growth to harden and provide extra support.
Overview
Adults with an acquired flatfoot deformity may present not with foot deformity but almost uniformly with medial foot pain and decreased function of the affected foot. Patients whose acquired flatfoot is associated with a more generalised medical problem tend to receive their diagnosis and are referred appropriately. However, in patients whose ?adult acquired flatfoot deformity? is a result of damage to the structures supporting the medial longitudinal arch, the diagnosis is often not made early. These patients are often otherwise healthier and tend to be relatively more affected by the loss of function resulting from an acquired flatfoot deformity. The most common cause of an acquired flatfoot deformity in an otherwise healthy adult is dysfunction of the tibialis posterior tendon, and this review provides an outline to its diagnosis and treatment.  Causes Many health conditions can create a painful flatfoot, an injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. Symptoms Many patients with this condition have no pain or symptoms. When problems do arise, the good news is that acquired flatfoot treatment is often very effective. Initially, it will be important to rest and avoid activities that worsen the pain. Diagnosis Your podiatrist is very familiar with tendons that have just about had enough, and will likely be able to diagnose this condition by performing a physical exam of your foot. He or she will probably examine the area visually and by feel, will inquire about your medical history (including past pain or injuries), and may also observe your feet as you walk. You may also be asked to attempt standing on your toes. This may be done by having you lift your ?good? foot (the one without the complaining tendon) off the ground, standing only on your problem foot. (You may be instructed to place your hands against the wall to help with balance.) Then, your podiatrist will ask you to try to go up on your toes on the bad foot. If you have difficulty doing so, it may indicate a problem with your posterior tibial tendon. Some imaging technology may be used to diagnose this condition, although it?s more likely the doctor will rely primarily on a physical exam. However, he or she may order scans such as an MRI or CT scan to look at your foot?s interior, and X-rays might also be helpful in a diagnosis. Non surgical Treatment There are many non-surgical options for the flatfoot. Orthotics, non-custom braces, shoe gear changes and custom braces are all options for treatment. A course of physical therapy may be prescribed if tendon inflammation is part of the problem. Many people are successfully treated with non-surgical alternatives.  Surgical Treatment Surgical intervention for adult acquired flatfoot is appropriate when there is pain and swelling, and the patient notices that one foot looks different than the other because the arch is collapsing. As many as three in four adults with flat feet eventually need surgery, and it?s better to have the joint preservation procedure done before your arch totally collapses. In most cases, early and appropriate surgical treatment is successful in stabilizing the condition. |
